A Case Report on Ethmoidal Sinus Metastasis: An Unusual Site of Metastasis in Periampullary Carcinoma Treated with Fsrt
A Case Report on Ethmoidal Sinus Metastasis: An Unusual Site of Metastasis in Periampullary Carcinoma Treated with Fsrt
Dr.Priya Sinha 1*, Dr.BKM Reddy2, Dr.Sairah Elizabeth Benny3
2. Radiation Oncologist.
3. Post Graduate student.
*Correspondence to: Dr.Priya Sinha, Apollo Hospital, Bannerghatta Road, Bengaluru.
Copyright.
© 2025 Dr Priya Sinha This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 May 2025
Published: 31 May 2025
DOI: https://doi.org/10.5281/zenodo.15621831
A Case Report on Ethmoidal Sinus Metastasis: An Unusual Site of Metastasis in Periampullary Carcinoma Treated with Fsrt
Introduction
Primary malignant neoplasm is more common than metastatic cancer in the paranasal sinuses(PNS) and are similar in presentations like recurrent epistaxis, nasal obstruction and facial pain. The most common site involved by metastasis is the maxillary sinus among the PNS. The most common site of metastasis in periampullary cancer is liver, lymph node, peritoneum, lung, bone. PNS metastasis in periampullary carcinoma is very uncommon.
Case Description
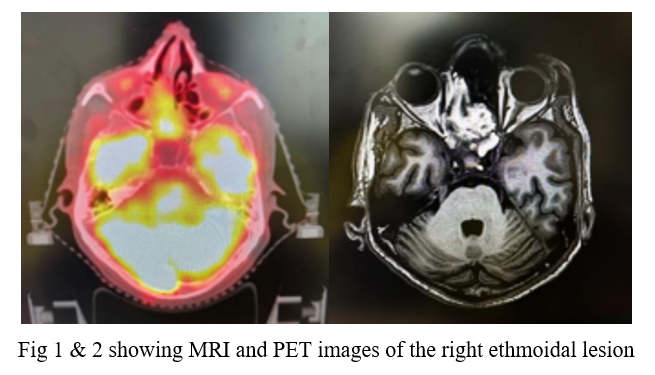
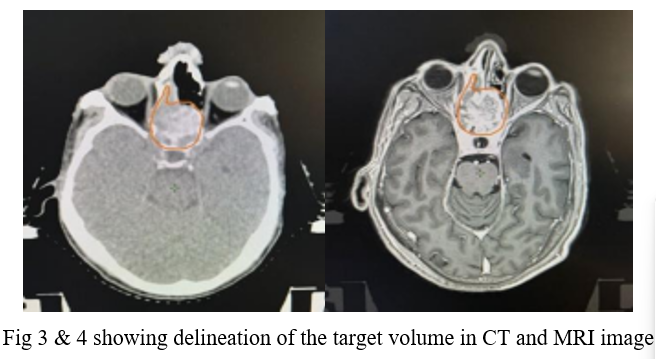
A 62-year old male, known case of periampullary carcinoma, presented with nasal bleeding since 15 days which was on and off and minimal in quantity. He had underwent whipples procedure followed by adjuvant chemotherapy. Later he presented with metastatic deposit in Lung for which he received chemotherapy. 3 years later, PET-CT scan showed increased uptake in lung nodules with local progressive disease and hypermetabolic uptake in right ethmoid sinus and planned for second line palliative chemotherapy. He presented with nasal bleed which was evaluated and confirmed by biopsy as metastatic adenocarcinoma. MRI of PNS showed heterogenously enhancing lesion involving the right ethmoid sinus, left posterior ethmoid, part of right nasal cavity and with a small extension into right frontal sinus, indenting right medial rectus muscle with involvement of adjacent pachymeninges. It measured 2.6x2.5cm with Max SUV6.2 on PET-CT scan. The metastatic deposit was managed by fractionated stereotactic radiation therapy(FSRT).The tumour was delineated with the help of MRI and PET-CT. He received 30Gy in 5 fractions, 1 fraction daily, using 6MV photons. After 4 months of treatment, there was no complaints of nasal bleeding, obstruction or headache.
Fig 1 & 2 showing MRI and PET images of the right ethmoidal lesion
Fig 3 & 4 showing delineation of the target volume in CT and MRI image
Discussion
Metastasis involving the ethmoid sinus is very rare. Renal cell carcinoma(RCC) is the most common primary tumour metastasising to PNS followed by breast, lung and prostate. Differential diagnosis of PNS metastasis includes wegners granulomatosis, midline granuloma and primary neoplasms. CT, and angiography may show soft tissue mass but biopsy is must for definitive diagnosis. Histologically adenocarcinoma the most commonly encountered cell type. Treatment in majority of the cases include chemotherapy and radiation therapy. In this case, our aim was to relieve him of symptoms from small sized lesion in a critically located site by a short course of radiation treatment, hence we chose FSRT. Mean survival time is 5-7 months with exception in case of RCC with PNS metastasis who can have 5 year survival as 15-30%.
Conclusion
PNS metastasis from periampullary carcinoma is rare with poor prognosis.As the metastatic deposit in the ethmoid sinus was symptomatic and located at critical site with impending extension to brain and eye, highly conformal with high dose per fraction(FSRT),palliative radiation was given in this case.
References
[1]. N.Azapira,M.J.Ashraf,B.Khademi et al.Distant metastasis to nasal cavities and paranasal sinuses case series.Indian J Otolaryngol Head Neck Surg.2011 Oct; 63(4):349-352.
[2] Francois Abi-Fadel,Peter R.Smith,Asim Ayaz et al.Paranasal sinus involvement in metastatic carcinoma.J Neurol Surg Rep.2012 Oct;73(1):57-59.
[3]Prescher A,Bros D.Metastasis to paranasal sinuses:case report and review of literature. Laryngorhinootologie. 2001;80:583-594.