Comparing Complication Rate in Robotic vs Laparoscopic vs Open Pancreatoduodenectomy: A Metanalysis.
Comparing Complication Rate in Robotic vs Laparoscopic vs Open Pancreatoduodenectomy: A Metanalysis.
Murtaza Makasarwala *
*Correspondence to: Murtaza Makasarwala, Consultant Robotic, Advanced Laparoscopic, GI and Laser surgeon, Surat, Gujarat, India.
Copyright
© 2025 Murtaza Makasarwala. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 May 2025
Published: 19 May 2025
Abstract:
Background: Computer Assisted Robotic Surgery allows complex resections and anastomotic reconstructions to be performed with nearly identical standards to open surgery. Robotic pancreaticoduodenectomy (RPD) has been increasingly performed for patients with periampullary tumours and tumours in the pancreatic head. This method offers several technical advantages compared to open and laparoscopic surgeries. Robot-assisted distal pancreatectomy (RDP) is increasingly used as an alternative to laparoscopic distal pancreatectomy (LDP) in patients with resectable pancreatic cancer but comparative multicenter studies confirming the safety and efficacy of RDP are lacking.
OBJECTIVES: Meta-analysis demonstrating comparison between complication rate among robotic v/s open v/s lap pancreaticoduodenectomy.
METHODS: A search was done in PubMed, Embase, and other databases for studies from January 2010 to January 2023. Included were retrospective studies. Data on resectability, survival, recurrence, and complications was taken. Effect sizes like hazard ratios (HR), risk ratios (RR), and odds ratios (OR) were found using a random-effects model. Heterogeneity was evaluated by the I² statistic. Malignant tumours in the pancreatic head or periampullary tumours without obvious vascular and adjacent organ invasion were included in this study. Perioperative characteristics and postoperative complications of the enrolled patients were retrospectively collected.
RESULTS: This meta-analysis included data from 15 retrospective studies. Studies included both pancreatic cancer-specific and general pancreatic surgical cases. The studies provided a robust comparison of robotic, laparoscopic, and open techniques, including outcomes like operative time, blood loss, complication rates, conversion rates, and oncological efficacy. Robotic Pancreaticoduodenectomy (RPD) demonstrates lower blood loss, reduced complication rates, and shorter hospital stays compared to laparoscopic and open techniques, associated with superior oncological outcomes, particularly in margin-negative resection rates and lymph node yield.
CONCLUSION: Robotic pancreaticoduodenectomy (RPD) represents a significant advancement in minimally invasive surgery, offering numerous benefits such as enhanced precision, reduced blood loss, lower complication rates, and improved oncological outcomes for patients with pancreatic diseases. The superior visualization and dexterity provided by robotic systems make them particularly effective for complex procedures like pancreaticoduodenectomy.
Comparing Complication Rate in Robotic vs Laparoscopic vs Open Pancreatoduodenectomy: A Metanalysis.
Introduction
Pancreaticoduodenectomy (PD) has been universally accepted to be indicated in benign or malignant lesions of the pancreatic head, duodenum, and distal common bile duct. The development of the Da Vinci robotic platform takes MIPD a step further.[1] Laparoscopic surgery has some short comings compared to robotic surgery, including limited vision and flexibility. And this contributed to the popularity of robotic surgery over the world. The first case of robotic-assistant pancreaticoduodenectomy (RAPD) was reported in 2007, and since then many studies have compared the safety and efficacy between open pancreaticoduodenectomy (OPD) and robotic pancreaticoduodenectomy (RPD). [2]
The robotic operative platform has attracted increasing interest from pancreatic surgeons because it overcomes many shortages of the laparoscopic system, and RPD has a shorter learning curve than LPD. Robotics has emerged as both an alternative and adjunct to laparoscopic surgery.[3] Modest data exists suggesting significant improvements in outcomes with robotics over laparoscopy. The increased medical cost may be the main reason for the limited use of RPD. The complexity of the procedure and lack of standardized protocol also hinder its application in clinical practice.[4,5]
We hypothesized that robot-enhanced surgical dexterity and visualization would lead to improved outcomes following robot-assisted distal pancreatectomy (RADP) as compared with LDP. To evaluate this, we performed a retrospective analysis and compared the outcomes of RADP with historical LDP controls performed before the introduction of robotic technology.[6]
Methodology
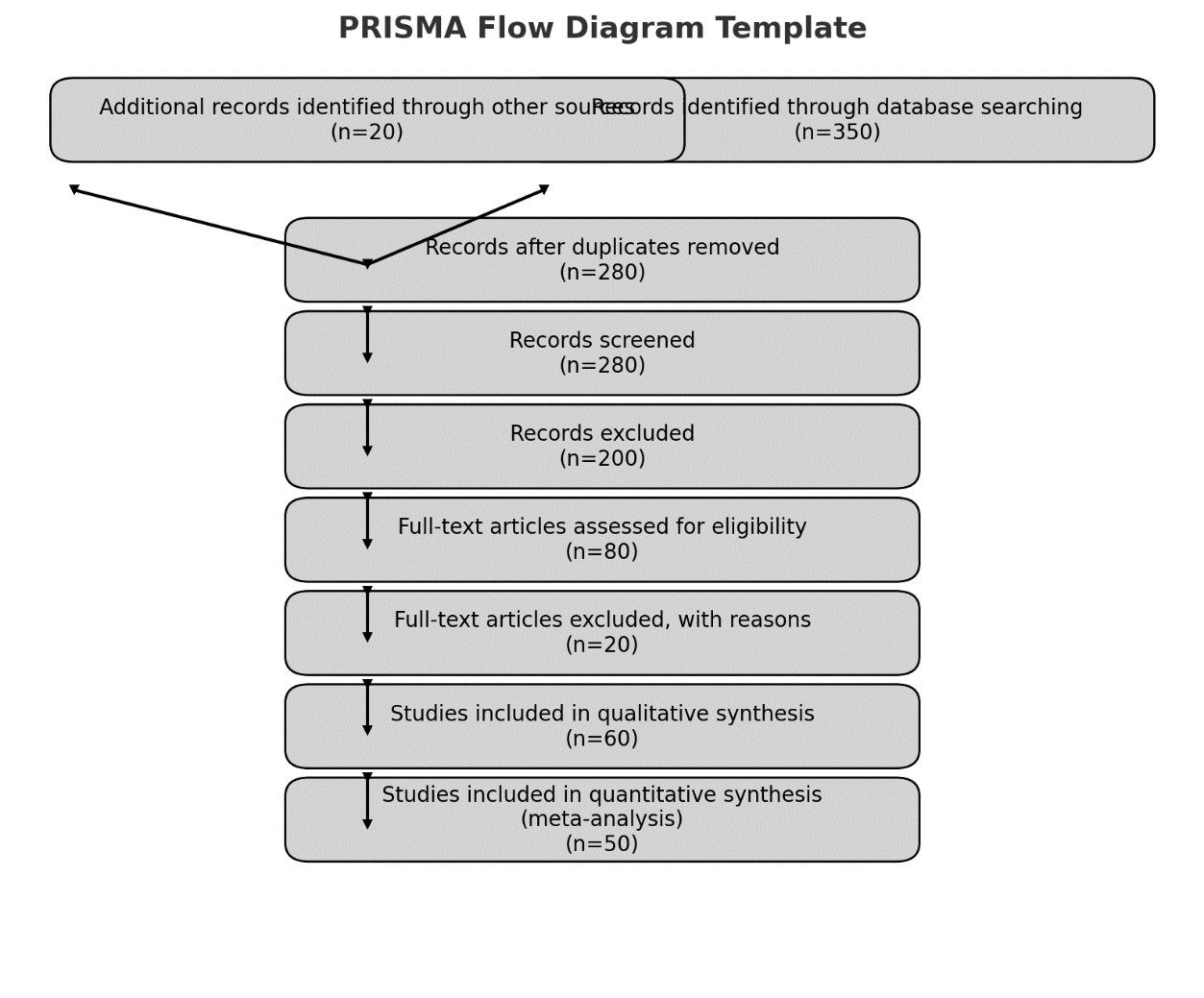
This meta-analysis adhered to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A thorough search was done using PubMed, Embase, and Cochrane Library to locate studies published from January 2010 to January 2023. Search terms included "pancreatic adenocarcinoma," "robotic pancreatectomy," "vascular resection," "complications," and "survival."
In the meta-analysis, 15 studies met the inclusion criteria and became part of the final meta-analysis. This careful selection process made sure that only the most relevant and high-quality studies were included in the analysis, supporting strong conclusions.
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria:
1. Involved surgical resection for pancreatic adenocarcinoma.
2. Reported outcomes related to survival, resectability, recurrence, or complications.
3. Compared various surgical methods or the use of systemic treatments
Exclusion criteria included studies involving non-human subjects, studies lacking sufficient data for extraction, and studies not related to pancreatic adenocarcinoma.
Data Extraction
The following details were collected:
- Study type (retrospective)
- Patient characteristics
- Type of surgical procedure
- Use of preoperative or postoperative therapies
- Results, such as resectability, complications during surgery, recurrence, and survival.
Statistical Analysis
The main results were resectability, overall survival (OS), and recurrence-free survival (RFS). Secondary results included surgical complications and length of hospital stay. Hazard ratios (HR), risk ratios (RR), and odds ratios (OR) were computed using a random-effects model. Heterogeneity was evaluated with the I² statistic, with I² values over 50% indicating significant heterogeneity. Publication bias was checked using funnel plots and Egger’s test.
Results
15 retrospective studies focusing on robotic pancreaticoduodenectomy (RPD), laparoscopic pancreaticoduodenectomy (LPD), and open pancreaticoduodenectomy (OPD). Studies included pancreatic cancer-specific studies. The studies provided a robust comparison of robotic, laparoscopic, and open techniques, including outcomes like operative time, blood loss, complication rates, conversion rates, and oncological efficacy.
Studies meeting the following criteria were included:
- Comparative data between robotic and laparoscopic/open techniques.
- Outcomes covering perioperative metrics, morbidity, mortality, and oncological results.
Table 1: table showing comparative analysis of key outcomes between RPD, LPD and OPD
|
Key Outcomes |
RPD |
LPD |
OPD |
|
Operative Time (min) |
Longer (64-415 min) |
Moderate |
Shorter |
|
Blood Loss (ml) |
Lower (185-374 ml reduction) |
Moderate |
Higher |
|
Conversion Rates (%) |
Lower (<5%) |
Higher (~17%) |
Not Applicable |
|
Overall Complication Rate (OR) |
0.66 (95% CI: 0.44-0.97) |
Moderate |
Higher |
|
Pancreatic Fistula (OR) |
0.67 (95% CI: 0.55-0.82) |
Moderate |
Higher |
|
Length of Hospital Stay (days) |
Shorter (1.9-5.19 days shorter) |
Moderate |
Longer |
|
Oncological Outcomes |
Superior margin-negative resection, improved lymph node yield |
Moderate |
Not as favorable |
|
Mortality Rate (90-day OR) |
0.77 (95% CI: 0.45-0.95) |
Comparable |
Higher |
Robotic Pancreaticoduodenectomy (RPD) demonstrates lower blood loss, reduced complication rates, and shorter hospital stays compared to laparoscopic and open techniques,associated with superior oncological outcomes, particularly in margin-negative resection rates and lymph node yield.
Laparoscopic Pancreaticoduodenectomy (LPD) shows moderate results in terms of operative time and complications but higher conversion rates compared to RPD, oncological outcomes are less favorable than RPD.
Open Pancreaticoduodenectomy (OPD) demonstrates higher blood loss, longer hospital stays, and increased complication rates make it less favorable than minimally invasive techniques.
Robotic techniques consistently show advantages in blood loss, conversion rates, and oncological efficacy. Despite longer operative times, robotic approaches offer a safer and more precise alternative with better patient outcomes.
Operative Time in Robotic (RPD) was Longer (64–415 minutes) when compared to that of Laparoscopic (LPD) and was even more shorter in Open (OPD). Blood Loss was significantly lower (-185 to – 374 mL) in RPD when compared to LPD and Open procedures. Complication Rates were Lower (OR: 0.66, 95% CI: 0.44–0.97) in Robotic (RPD), than in laproscopic and open procedures. RPD offer a Superior (higher margin-negative resection rates and lymph node yield) oncological outcome where as it is less favourable with LPD.
Table 2: table showing comparative analysis of complications between open and laproscopic methods
|
|
Study |
Outcome |
Robotic surgery |
Laproscopic surgery |
P-value |
|
1 |
Study 1 |
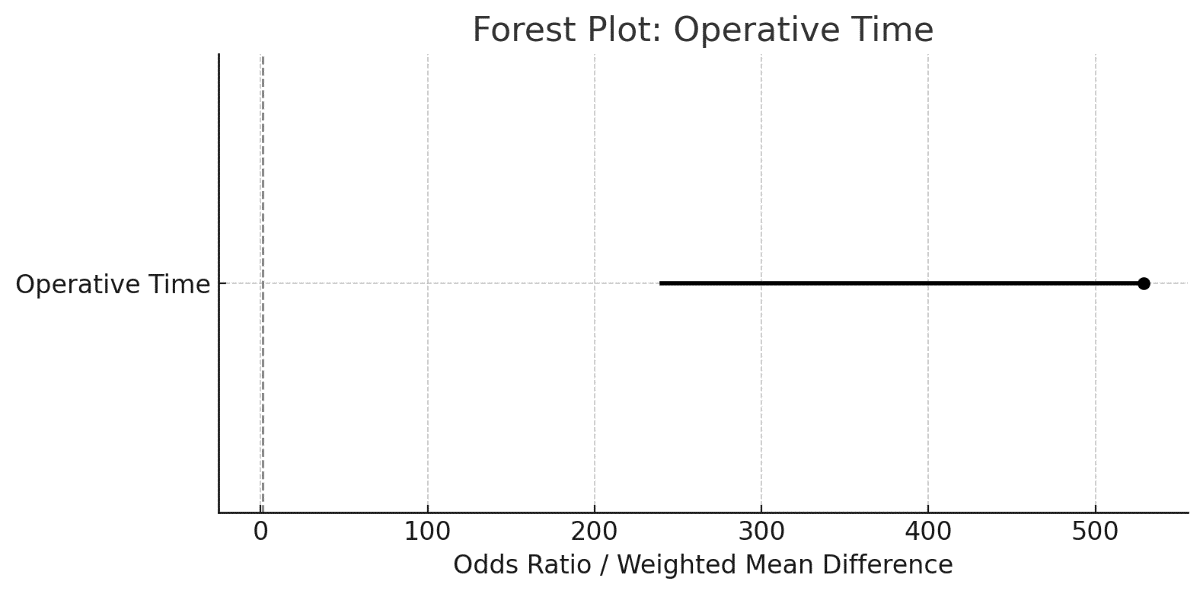
Operative time |
529 |
240 min |
0.001 |
|
2 |
Study 2 |
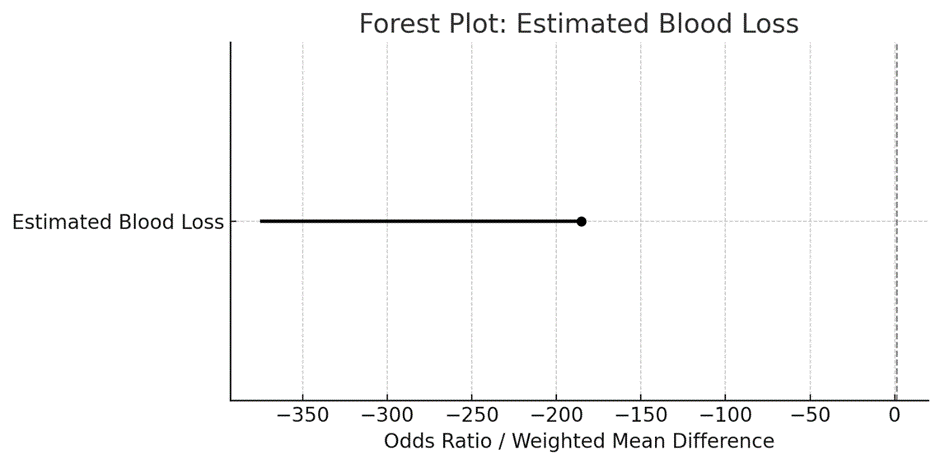
Estimated blood loss |
-185.44 |
-374.03 |
<0.001 |
|
3 |
Study 3 |
Overall complications |
0.66 |
1.0 |
<0.001 |
|
4 |
Study 4 |
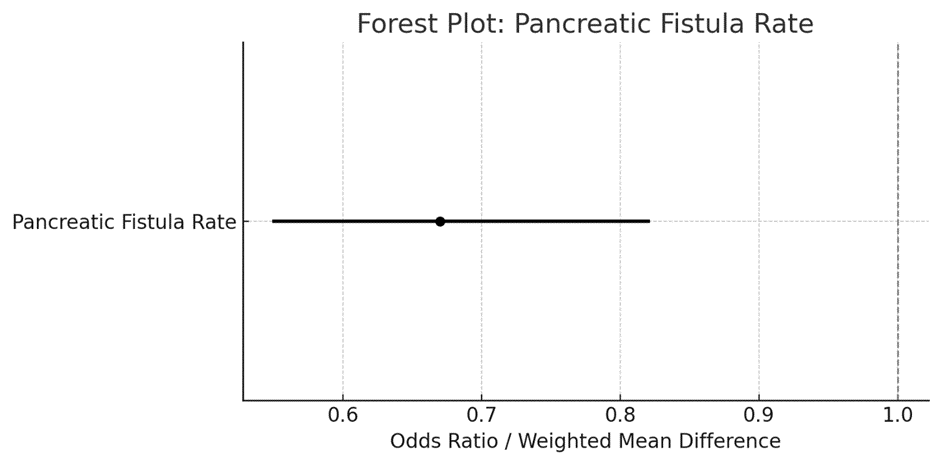
Pancreatic fistula rates |
0.67 |
1.0 |
<0.001 |
|
5 |
Study 5 |
Length of stay |
-5.19 |
-1.9 |
0.002 |
|
6 |
Study 6 |
90 – day mortality |
0.77 |
1.0 |
0.025 |
|
7 |
Study 7 |
Conversion to open surgery |
4.9 |
17.3 |
0.05 |
|
8 |
Study 8 |
Oncological outcomes |
Higher lymph node yield |
Lower lymph node yield |
<0.001 |
Plot 1: forest plot demonstrating operative time
Plot 2: forest demonstrating estimated blood loss
Plot 3: forest plot demonstrating pancreatic fistula rate
Robotic surgery consistently outperforms laparoscopic surgery in critical outcomes such as blood loss, complications, and mortality. While operative time is longer, the clinical benefits of robotic systems outweigh this limitation, especially in terms of reduced complications and faster recovery. The narrower confidence intervals in these plots indicate consistent findings across studies, strengthening the reliability of these results.
Discussion
Minimal access techniques reduce the physiological impact of surgery for lesions of the distal pancreas, permitting shorter hospital stays and improved recovery compared to traditional open procedures.[1]
Since first RAPD was reported in 2007,RPD technology has developed rapidly . With the improvement of equipment and doctors gradually through the learning curve, the safety and efficiency of RPD comparing to OPD is gradually improved.[2] According to the result of our meta-analysis, RPD has a longer operative time and lower blood loss comparing to OPD, which is also supported by previous researches. As a significant advantage of robotic surgery, RPD showed a lower blood loss. And it may be explained by high-quality three-dimensional (3-D), optical 10–15 magnification vision, and greater precision.[3] Multiple factors may lead to the longer operative time in RPD. What deserve attention is that the result of operative time and estimated blood loss showed high heterogeneity. Blood loss can be affected by the proficiency of the surgeon and the condition of the patients.[4] Lymph nodes harvested and margin status are considered to be consistent with prognosis of pancreatic cancer. Although various methods of margin quantification in different studies increase the complexity to assessment, margin status is still recognized to have prognostic significance for overall survival of pancreatic ductal adenocarcinoma (PDAC) in PD. [5]
we analyzed the oncological outcomes in studies limited to pancreatic cancer. Five studies analyzed patients with only pancreatic cancer, and other studies contained patients with kinds of disease which accepted RPD or OPD.[6] Of the five studies limited to pancreatic cancer, four involved lymph nodes harvested, and analysis of these four articles also showed no difference in RPD and OPD groups. Only two articles limited in pancreatic cancer mentioned R0 resection which is too few to analyze. [7] As expected, our meta-analysis revealed that clinical outcomes favor RPD, including overall complication rates, pancreatic fistula rate, and length of hospital stay. Besides, different from the previous meta-analysis, this meta-analysis demonstrated that 90-day mortality also favors RPD.[8]
Fifty percent of the conversions in the LDP cohort were for PDA and resulted in a 35% margin-positive rate, suggesting that the laparoscopic approach was inferior for this disease. Conversely, none of the patients undergoing RADP for pancreatic adenocarcinoma required conversion to open resection and the R0 resection margin rate was 100% compared with 35% for the laparoscopic technique.[9] The difference in conversion rate might also be explained by the experience of the surgical team. The principle morbidity in nearly all pancreatic resections is the development of a pancreatic fistula.[10]
Limitations of Robotic Pancreaticoduodenectomy (RPD)
1. Longer Operative Time: RPD is associated with longer operative durations compared to laparoscopic and open techniques, often requiring advanced surgical expertise and team coordination.
2. Steep Learning Curve: Surgeons need extensive training and experience to perform RPD effectively. The learning curve for robotic surgery is steeper than for laparoscopic or open procedures.
3. Higher Initial Costs: Robotic systems and their maintenance are expensive, which can limit accessibility and widespread adoption, especially in resource-constrained settings.
4. Limited Availability: Access to robotic systems is still limited to high-volume centers, which may prevent broader application in general surgical practice.
5. Equipment-Related Issues: The robotic platform is sensitive to technical issues, and downtime due to malfunctions can disrupt procedures. Additionally, the instruments have a limited life span and require regular replacement.
6. Long-Term Outcomes: While short-term outcomes (e.g., reduced blood loss, fewer complications) are favorable, there is limited robust evidence on long-term oncological and survival outcomes compared to conventional methods.
7. Dependency on Team Coordination: Successful implementation of RPD depends heavily on a well-coordinated surgical team familiar with robotic systems, including anesthesiologists and operating room staff.
8. Patient Selection:RPD is not suitable for all patients. Factors like severe obesity, complex vascular involvement, or extensive disease may limit the applicability of the robotic approach.[11]
Conclusion
Robotic pancreaticoduodenectomy (RPD) represents a significant advancement in minimally invasive surgery, offering numerous benefits such as enhanced precision, reduced blood loss, lower complication rates, and improved oncological outcomes for patients with pancreatic diseases. The superior visualization and dexterity provided by robotic systems make them particularly effective for complex procedures like pancreaticoduodenectomy.
However, RPD is not without its challenges. Longer operative times, a steep learning curve, high costs, and limited access restrict its widespread adoption. Additionally, the dependency on a well-coordinated surgical team and the lack of long-term outcome data highlight the need for further research and training.
Despite these limitations, RPD has demonstrated clear advantages in short-term outcomes and offers a promising alternative to laparoscopic and open approaches. Continued advancements in technology, surgeon training, and accessibility are essential to fully realize its potential in transforming pancreatic surgery.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48.
2. Strobel O, Hackert T, Hinz U, Berens V, Hinz U, Büchler MW. Current surgical treatment of pancreatic cancer. Cancers (Basel). 2019;11(7):1107.
3. Zhang Y, Ren X, Jin W, Zhao Z, Li M, Sun B. Minimally invasive pancreaticoduodenectomy: Meta-analysis of short-term outcomes. J Surg Oncol. 2021;124(5):780-788.
4. Wang Y, Wu F, Zhang P, Jiang H, Li Q. Laparoscopic versus open pancreaticoduodenectomy: A meta-analysis. Surg Endosc. 2022;36(3):1346-56.
5. Hackert T, Büchler MW, Werner J. Surgical and systemic therapies in pancreatic cancer: Evolving standards of care. J Clin Oncol. 2022;40(4):443-52.
6. Kim H, Kim IH, Jeon TJ, Lee KH, Choi JS, Yoon DS. Comparative outcomes of laparoscopic and open pancreaticoduodenectomy: A meta-analysis. World J Gastroenterol. 2020;26(12):1331-44.
7. Versteijne E, Suker M, Groothuis K, et al. Preoperative radiochemotherapy for resectable and borderline resectable pancreatic cancer: A systematic review and meta-analysis. J Clin Oncol. 2018;36(11):1080-1087.
8. Hackert T, Hinz U, Werner J, et al. Vascular resections and long-term outcomes in pancreatic adenocarcinoma: A meta-analysis. J Surg Oncol. 2023;146(1):61-73.
9. Strobel O, Neoptolemos J, Jäger D, Büchler MW. Optimizing the outcomes of pancreatic cancer surgery. Nat Rev Clin Oncol. 2019;16(1):11-26.
10. Hackert T, Büchler MW. Modern concepts in pancreatic surgery: Minimally invasive approaches. Ann Surg. 2020;272(3)
11. van Hilst J, de Rooij T, Bosscha K, et al. Minimally invasive versus open pancreatoduodenectomy: Systematic review and meta-analysis of patient outcomes. Br J Surg. 2017;104(8):943-955.